
People in Northern Ireland can now expect to live into their late seventies and early eighties, yet only to around age 60 in good health. This means many spend close to two decades living with illness or disability, with even longer periods of poor health in the most deprived communities. What was once viewed primarily as a public health statistic is now shaping budgets, workforce pressures and the long‑term sustainability of public services.
A growing health gap
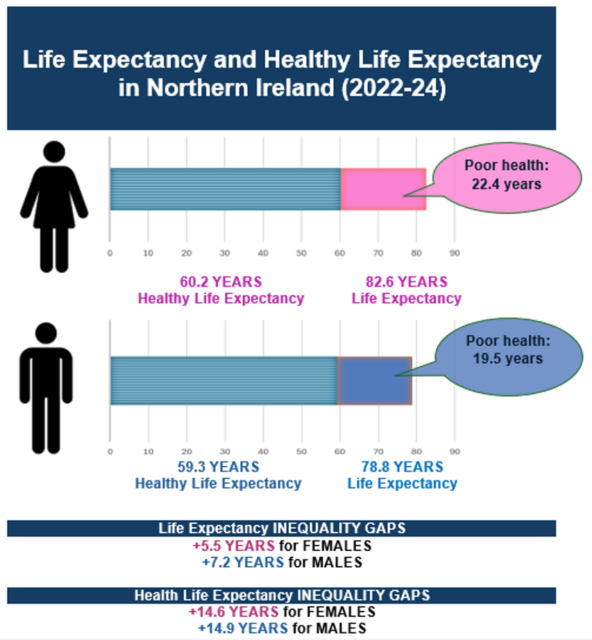
Across the UK, gains in life expectancy (LE) have slowed, while healthy life expectancy (Healthy LE) has stalled or declined. Northern Ireland reflects this pattern but with a more pronounced divide: people are living longer, yet a substantial share of those additional years is spent in poor health. Recent Department of Health figures (December 2025) show that in 2022–24, LE in Northern Ireland was 78.8 years for men and 82.6 years for women, while Healthy LE was much lower at 59.3 and 60.2 years respectively.
The gap is widest in deprived areas, where illness begins earlier and lasts longer. LE differs by around six years between the most and least deprived communities, but the gap in healthy years is more than double that, at nearly 15 years for both men and women. Recent trends suggest this divide is widening, particularly for men: over the past five years, Healthy LE has fallen by 1.9 years for women and 0.8 years for men, while the male deprivation gap in Healthy LE has increased from 12.0 to 14.9 years.
Geographical variation adds another layer. In Lisburn & Castlereagh, men live on average to 80.5 years and women to 83.8 years, compared with 76.5 and 80.5 years respectively in Belfast.
These patterns echo what Professor Sir Michael Marmot, keynote speaker at NICON25, Northern Ireland’s flagship conference for health and public‑sector leaders, describes as the ’causes of the causes’: income, education, work, housing, early childhood experiences and the wider environment.
Addressing senior officials and system leaders, he emphasised that these structural conditions shape not only how long people live, but how long they live in good health.
This reality is already visible across Northern Ireland. People in the most deprived communities not only die younger, they spend more of their lives in poor health. The same pressures that hold back LE also bring illness earlier, widening the gap in healthy years. Other inequalities intersect with deprivation, compounding disadvantage. Women typically live longer but often spend more years in poor health, influenced by caring responsibilities, musculoskeletal conditions and depression. Rural communities experience ‘hidden deprivation’ through limited transport, fuel poverty and reduced access to services. Ethnicity and migration also shape people’s access to support and their experience of the system.
Taken together, these overlapping inequalities reinforce a central message from NICON25: closing the health gap requires coordinated action across government, not solely within the health and social care system.
Why it matters
LE reflects how long people are expected to live if current trends continue. Healthy LE considers how many of those years are likely to be spent in ‘good’ health, free from long‑term conditions or disability, based on people’s own reports in surveys. The map below brings these disparities into sharp focus, tracing how LE has shifted over time while revealing the electoral districts where deep‑rooted inequalities continue to persist.
An interactive map showing life expectancy through time broken down for males and females, by District Electoral Area (DEA); click on any DEA to view its results alongside the Northern Ireland average. The map can also be accessed directly here
________________________________________________________________________
Healthy LE is not simply a public health statistic: it influences budgets, productivity, and demand across health, social care, and wider public services. This is why Northern Ireland’s Programme for Government tracks HLE and the HLE inequality gap as key indicators.
Why the gap exists and how NI compares
High rates of chronic illness in deprived areas, long waiting times that exacerbate conditions, and wider social factors such as housing, education and employment all contribute to drive poorer health outcomes. These challenges combine with modifiable risks such as smoking, alcohol use, poor diet and low physical activity to further drive ill health.
According to the Department of Health’s Health Inequalities Annual Report 2025, respiratory deaths among those under 75 are almost three‑and‑a‑half times higher in the most deprived areas, and mental health inequalities remain marked, with prescription rates for mood and anxiety disorders two‑thirds higher than in the least deprived. Suicide mortality is nearly three times higher, while drug misuse deaths show the largest gap, with rates almost six times those in the least deprived communities. Smoking in pregnancy, teenage births and childhood obesity also remain among the widest deprivation gaps, highlighting the persistence of health inequalities across Northern Ireland. These patterns point to solutions that must extend well beyond clinical care and into the social determinants of health.
These trends align with a broader UK pattern of ‘partial expansion of morbidity’: people are living longer, but more of those years are spent managing illness. Northern Ireland stands out because the years spent in poor health form a larger share of total LE than in most other UK nations, and its deprivation‑related Healthy LE gap is particularly marked.
Deprivation gaps in LE are slightly narrower than in Scotland or England, but gaps in Healthy LE remain substantial. They are smaller than the very wide gaps observed in some Scottish and Welsh areas, yet still point to deep inequalities within Northern Ireland.
However, direct comparisons across the UK and the Republic of Ireland require caution, as differences in survey methods, time periods and deprivation measures can distort the picture. This was evident in a recent media report suggesting that people in the Republic of Ireland enjoyed almost a decade more healthy life than those in Northern Ireland; once methods were aligned, the difference narrowed to less than 2 years.
From rising demand to policy levers
Inequalities translate into rising demand for health and social care (H&SC) services. Ageing plays a role, but it is only one part of a wider set of pressures. Three dynamics appear particularly influential:
- A larger older population: Growth in the number of people aged 65 and 85 is associated with higher levels of chronic illness and frailty. Although LE has recovered, many of the additional years are not healthy ones, placing sustained pressure on Health and Social Care services.
- Earlier onset of illness in deprived areas: People in the most deprived communities tend to develop limiting conditions a decade or more earlier than those in more affluent areas. This contributes to higher Health and Social Care service use at younger ages and is linked to economic inactivity and reliance on welfare.
- The normalisation of multimorbidity: Many older adults, and increasing numbers in midlife, live with multiple conditions. When primary and community services are stretched, people are more likely to present in crisis, adding to pressure on emergency departments and hospital beds.
These pressures are reflected in waiting lists and budgets. Currently, Northern Ireland has the longest waiting lists in the UK, with delays driven not only by pandemic backlogs but from sustained demand for Health and Social Care services associated with an ageing population living longer in poor health. Financial overspends often point to a mismatch between need and system design rather than inefficiency. Structural productivity constraints, outdated infrastructure, high unit costs and excess bed days all suggest that capital investment and modernisation sit alongside workforce planning as key considerations. It was against this backdrop that, in May 2025, the Health Minister announced a series of waiting list initiatives and an updated Elective Care Framework Implementation and Funding Plan, setting out new measures and targeted areas of investment intended to address these systemic pressures.
Northern Ireland’s policy framework acknowledges these challenges. As mentioned, the Programme for Government tracks Healthy LE and inequality gaps, while the Belfast Agenda highlights reducing health inequality as a core priority within its long-term vision for 2035, with partners committed to improving outcomes across the city’s most deprived neighbourhoods.
These pressures form the backdrop to the strategic direction set out in the Department of Health’s Reset Plan. This plan, reaffirmed at NICON25, highlights a ‘shift left’ toward prevention, early intervention and community‑based care. Yet spending remains heavily weighted toward acute services, making it difficult to redirect resources upstream. While early improvements in elective care are emerging, prevention continues to struggle to gain momentum in a context where acute pressures dominate day‑to‑day decision‑making.
Closing the gap: Execution and system change
Translating strategy into impact appears to rely on a blend of place‑based and system‑wide activity. A number of practical approaches are already emerging, including neighbourhood‑level models such as Live Better, the continued rollout of multidisciplinary teams (MDTs) in primary care, expansion of community diagnostics and screening, and the strengthening of behavioural‑risk measures, for example, efforts to reduce smoking and vaping and ongoing consideration of Minimum Unit Pricing for alcohol, alongside early‑life interventions. These developments are intended to support progress in compressing morbidity and reducing inequality. Achieving this at scale, however, continues to be shaped by structural pressures, particularly the persistent pull of acute‑care demand, which can limit the capacity to invest in preventive and community‑based services.
For Northern Ireland, the key challenge is not defining ambitions but supporting their consistent delivery across the system. Measures such as Healthy LE and its inequality gradient are already embedded within the Programme for Government, and there are indications that giving these metrics greater prominence within system discussions could help strengthen the link between monitoring and improvement. Given the Reset Plan’s emphasis on prevention and reducing inequalities, metrics such as Healthy LE and the deprivation gap are sometimes highlighted as potential indicators that could help signal priority and support alignment across the system. England has committed to improve Healthy LE by 5 years by 2035, and to halve the gap between the healthiest and least healthy, a commitment often referenced as an example of how targets can encourage a shift toward prevention and community‑based care, though the effectiveness of such approaches continues to be assessed.
Attention has also focused on deprivation. Evidence consistently shows that prevention and community support tend to have the greatest impact in areas with the poorest LE and Healthy LE, particularly when guided by mapped data. These pressures have led many analysts to highlight the importance of sustained investment in prevention rather than short‑term pilots. Wider UK work has explored mechanisms such as protecting prevention budgets or gradually increasing them over time, including models that reinvest a share of acute‑care savings into upstream interventions. Such approaches align with Northern Ireland’s emphasis on prevention, even if they are not yet formalised within local policy. These conversations sit alongside the practical measures already signalled across the system.
Recent analysis has further highlighted the importance of rebalancing workforce and infrastructure. A future in which more care is delivered in homes and communities, and where a greater share is social as well as medical, is likely to involve shifts in staff mix, for example, more community nurses, allied health professionals and social care workers, and changes in the types of facilities required, with fewer long‑stay acute beds and greater emphasis on step‑down and intermediate care.
Following Marmot’s observation that ‘social injustice is killing on a grand scale‘, many analyses point to the need for action that extends beyond the Department of Health. Housing, income security, education, employment and transport all influence both LE and Healthy LE, suggesting that efforts to reverse the expansion of morbidity sit within a wider policy landscape. In this view, compressing morbidity becomes a whole‑of‑government endeavour, with health equity embedded across departmental decision‑making. There is also growing recognition that interventions developed with communities, rather than solely for them, tend to be more effective, particularly in areas facing higher levels of deprivation. Co‑production is frequently referenced within Northern Ireland’s existing approaches, from neighbourhood‑level planning to regional strategies.
Measuring progress: Health, not just longevity
A substantial body of evidence shows that unequal societies not only shorten lives but also concentrate ill health among those with the fewest resources, and Northern Ireland reflects this pattern. LE has returned to around 78.8 years for men and 82.6 for women, yet Healthy LE remains close to 60 years, leaving nearly two decades lived in poor health, and even more in the most deprived communities.
If the expansion of morbidity is shaped by social and economic inequality, clinical advances on their own are unlikely to reverse it. Treating individuals and then returning them to the circumstances that contributed to their ill health does little to shift long‑term outcomes.
A more hopeful trajectory, reflected in several existing plans, involves a deliberate focus on compressing morbidity by addressing the social determinants of health and reducing modifiable risks such as smoking, alcohol use, poor diet and low physical activity. This points towards a system that invests earlier in the life course, anticipates the needs of an ageing population and directs attention to areas where disadvantage is most concentrated.