
Northern Ireland’s Health and Social Care system is balancing the demands of today alongside the reforms needed for tomorrow. As waiting times in Northern Ireland remain significantly longer than elsewhere in the UK, and services work tirelessly to meet daily demand, the Department of Health is poised to launch one of the most significant programmes in recent decades, the Neighbourhood Model of Health and Wellbeing, scheduled to begin implementation in April 2026.
The model seeks to bring care closer to home, strengthen community provision, and rebalance the system to reduce over-reliance on acute hospitals. Importantly, it extends beyond healthcare alone, placing equal emphasis on prevention, social care, wellbeing, and the wider determinants of health. Yet it arrives at a time of extraordinary pressure. Progress in these circumstances will be challenging, and the benefits of neighbourhood working will take time to accumulate. The gap between today’s demands and tomorrow’s ambitions is therefore real, and understanding how to navigate it is central to the success of this reform.
Why change, why now?
Northern Ireland’s health and social care system continues to absorb pressures that stretch far beyond hospital waiting lists alone. As demand rises and demographics shift, the consequences are felt on both sides of the system. For service users, this means increasingly uneven access to healthcare, longer waits, and care that can feel fragmented as people move between siloed services not always designed to work together. These pressures contribute to poorer outcomes, particularly for those living with long‑term conditions or in communities facing socioeconomic disadvantage, and they erode confidence in a system striving to respond to needs that present earlier, more frequently, and with greater complexity.
For those delivering care, the impact is equally significant. Workforce satisfaction is affected as staff operate in environments shaped by rising demand, higher administrative burden and the duplication that comes from services working in isolation. Costs increase, communication can become more challenging, and opportunities to work efficiently across organisational boundaries are harder to realise. These pressures accumulate and, taken together, raise important questions about long‑term sustainability. In this landscape, the case for a different model of working becomes clearer: one that reduces fragmentation, supports collaboration, and enables services to intervene earlier, before people reach crisis point and before pressures overwhelm the system’s capacity to respond.
What is the Neighbourhood Model?
The Neighbourhood Model is built on a simple but transformative idea: organising care around people and places rather than institutions. It aligns with international approaches and reflects commitments already signalled in Delivering Together, Health and Social Care NI – A Three Year Plan to Stabilise, Reform and Deliver , and the Health and Social Care NI Reset Plan.
It is explicitly framed as a neighbourhood model of health and wellbeing, integrating healthcare, social care, community services and prevention, rather than a standalone service reconfiguration. Importantly, Integrated Neighbourhood Teams are not new statutory organisations but provider alliances operating within existing accountability, planning and funding arrangements.
Its aims include:
- Bringing more care closer to home
- Improving access and continuity in general practice
- Strengthening community services
- Enabling integrated, proactive care for those with complex needs
- Reducing avoidable hospital use
- Supporting prevention and early intervention
- Engaging communities as partners
The policy framework makes clear that this approach is underpinned by four equally important pillars. Together, these aims reflect an intentional shift from episodic, service‑led responses to a population‑based, preventative model grounded in neighbourhoods:
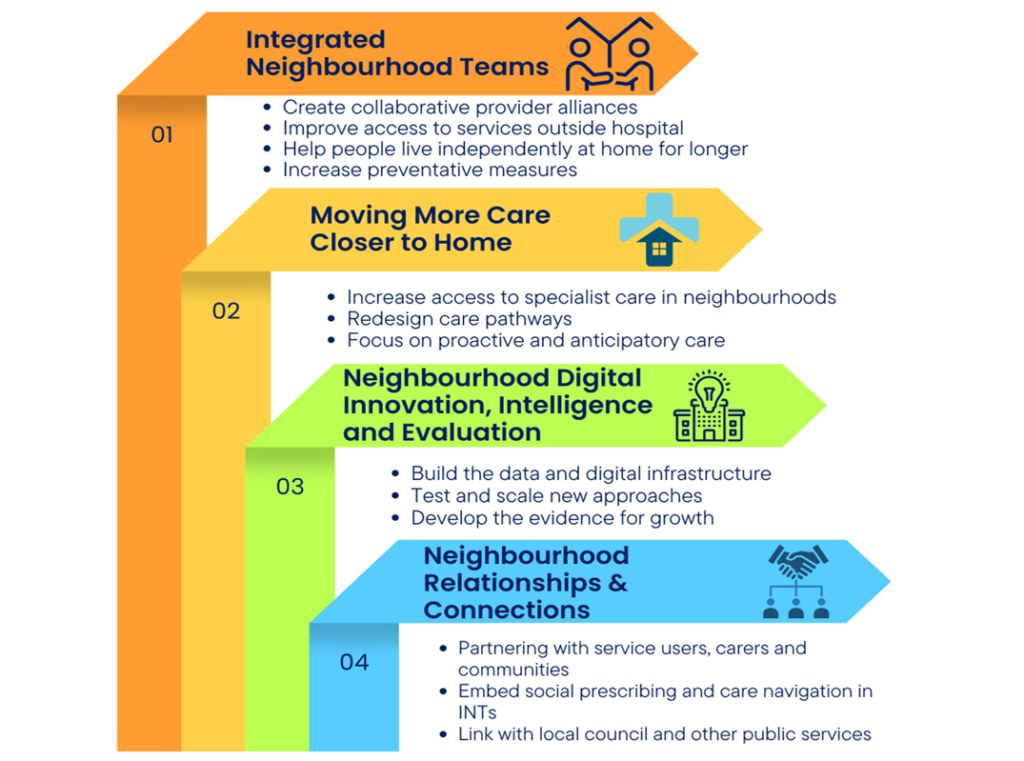
Together, these pillars are intended to ensure the model is not simply a structural reorganisation, but a supported, data‑enabled and continuously improving approach to neighbourhood health and wellbeing.
Evidence from neighbourhood models elsewhere is promising but mixed. Many report improved access, stronger collaboration and better engagement with under-served groups. At the same time, challenges such as funding constraints, digital immaturity and limited evaluation frameworks are common. The Northern Ireland model draws explicitly on these lessons, seeking to embed digital capability, data and evaluation from the outset.
How will it work in Northern Ireland?
The HSC Reset Plan sets out the establishment of 17 Integrated Neighbourhood Teams (INTs), each serving populations of around 115,000. These INTs will function as provider alliances, drawing together:
- GPs and GP Federations
- Community pharmacy
- Trust‑delivered community services
- VCSE organisations
- Independent providers
- Local government and other statutory partners
Implementation will follow three phases:
- Design (completed January 2026)
- Build (to April 2026)
- Implementation (from April 2026, with INTs established progressively and developing at different paces depending on local readiness)
The Policy Framework is explicit that early implementation will focus initially on older people, reflecting demographic ageing, higher levels of need, and the pressure this places on health and social care services. This life‑course approach is intended to expand over time as neighbourhood capacity builds.
The model is supported by a mixed funding approach. While it does not rely on large new baseline funding, it is underpinned by the redirection of existing resources, targeted transformation funding, and invest‑to‑save approaches. From 2026/27, the Department has committed to progressively shifting up to 2% of hospital‑based spend annually into community provision, alongside enabling investment in digital, workforce and neighbourhood infrastructure.
This reflects the long‑term direction set since Bengoa, ‘shifting left’ toward prevention and early intervention, but it unfolds within a financial environment that remains highly constrained. Within these constraints, INTs are expected to develop in ways that reflect local identity and need, creating neighbourhoods ‘small enough to feel local, but big enough to make a difference’.
What can we learn from elsewhere?
Neighbourhood models across the UK and internationally offer a body of emerging, albeit imperfect, evidence. A growing evidence base and synthesis of neighbourhood working identifies key enablers: strong local leadership, multidisciplinary configuration, shared purpose, and robust partnerships. It also highlights the typical pitfalls: digital fragmentation, short‑term funding and inconsistent evaluation.
Other analyses emphasise the importance of aligning community assets with statutory services, stable governance, and approaches sensitive to local inequalities. The Northern Ireland model explicitly seeks to address these weaknesses through neighbourhood‑level governance, data frameworks and structured development support.
The Nuka System of Care in Alaska demonstrates the impact of community‑owned, prevention‑focused services on long‑term population health. In New Zealand, the Canterbury model illustrates how integrated working across hospital, primary and community services can develop rapidly when leadership and shared purpose align. Closer to home, Wigan’s asset‑based approach and the Manchester Primary Care model show how local partnerships, proactive care and strong community infrastructure can help reshape demand and support earlier intervention. These examples reinforce that neighbourhood working is both practical and achievable when relationships, trust and local flexibility are prioritised.
What makes neighbourhood working measurable and sustainable?
Digital capability, data and evaluation are not treated as optional enablers within the Neighbourhood Model but as core infrastructure for change. The Policy Framework proposes a neighbourhood‑level data and intelligence framework, bringing together population health needs, service activity and indicators of inequality to inform planning and proactive care.
INTs will be supported with shared digital platforms, secure information‑sharing arrangements and improvement capability, enabling teams to:
- Identify high‑risk groups earlier
- Coordinate support across organisational boundaries
- Measure outcomes at neighbourhood level
- Test, refine and scale new ways of working
This focus responds directly to the shortcomings of earlier place‑based initiatives, where promising approaches often struggled to evidence impact or move beyond pilot phases due to limited digital maturity and evaluation capacity.
How do we create the conditions for long-term change?
Building on these enabling foundations, embedding neighbourhood working at scale requires attention to a wider set of system conditions over time. Northern Ireland is well‑positioned in terms of ambition and design. Crucially, the model positions citizens, service users and carers not as passive recipients of care, but as partners within neighbourhood teams and neighbourhood design, bringing lived experience into planning, delivery and evaluation. But doing so at scale requires careful navigation through several evolving areas: constrained budgets, workforce pressures, digital systems that continue to mature, and the need for neighbourhood‑level outcomes frameworks and meaningful community engagement.
It is equally important to recognise that prevention works differently from acute interventions. Its effects are gradual and cumulative, becoming visible over years rather than months. This longer timeline has historically made prevention harder to appraise in economic modelling, which often undervalues long‑term population benefits and rarely captures the broader social impact of neighbourhood‑based care. For this reason, the evidence base is still emerging, not because prevention is uncertain, but because outcomes take time to mature.
Yet delaying this shift also carries a cost. Neighbourhood working has the potential to create a virtuous cycle: healthier communities, fewer crises, reduced pressure on acute services, and more capacity to reinvest upstream. This progress will be incremental, but it must begin now.
How can Northern Ireland build on its existing strengths?
The Department of Health’s Call for Evidence highlighted that neighbourhood working already exists across Northern Ireland, even if not formally recognised as such. Examples include:
Voluntary, Community and Social Enterprise (VCSE) led social prescribing
Neighbourhood‑embedded initiatives supporting mental health, long‑term conditions, and family wellbeing, particularly in more deprived areas.
Healthy Living Centres
Acting as local anchors that bridge health, housing, employment and advice services.
Live Better demonstration sites
In Belfast and Derry/Londonderry, these initiatives showcased co‑production and neighbourhood‑specific design.
Early Place Based Partnership Models
GP-pharmacy-VCSE collaborations, community‑development approaches, and locally targeted support around the social determinants of health.
Multidisciplinary collaboration
Examples of cross‑sector early intervention and use of community infrastructure to provide more advanced services closer to home.
These initiatives informed the design of the Neighbourhood Model and demonstrate that Northern Ireland is not starting from scratch, but formalising and scaling what already works.
Why does timing matter more than ever?
Timing remains one of the most complex dimensions of reform. Acute services are under pressure now, while neighbourhood working delivers benefits gradually. The Policy Framework recognises this tension and positions neighbourhood working not as a substitute for stabilising acute services, but as a necessary companion to long‑term sustainability.
These are not competing demands. They are mutually reinforcing. Neighbourhood models require sustained commitment, iterative learning and the patience to allow gradual improvements to accumulate.
What can we learn from other place-based approaches?
These timing pressures also help explain why some stakeholders remain sceptical of the Neighbourhood Model. While neighbourhood and place‑based initiatives have existed across Northern Ireland for some time, policy reviews and engagement feedback indicate that they were often limited in scale, reliant on short‑term funding, and insufficiently embedded in system‑wide structures to sustain impact. Where promising approaches did emerge, they were not consistently embedded into mainstream commissioning, leading to lost momentum rather than demonstrable failure. Scepticism therefore reflects less a rejection of neighbourhood working itself than concern about whether the system can now provide the stability and follow‑through required for it to take root at scale.
How does implementation pace shape long-term outcomes?
Northern Ireland is entering a challenging but necessary phase of reform. The Neighbourhood Model offers a practical, evidence‑informed approach to shifting care closer to home and strengthening prevention, even amid significant pressures. It reflects long‑standing commitments and aligns with what communities repeatedly say they want.
The conditions for change are not ideal. Budgets are stretched, services under pressure, and digital systems still evolving. But these realities also underscore why the ‘shift left’ cannot be postponed. As noted at the NICON24 conference two years ago, there comes a point when the system must ‘grasp the nettle’: acknowledging that, while the context is difficult, the cost of waiting is greater.
The immediate task is to begin building the neighbourhood infrastructure that will support improvement over time. Progress will undoubtedly be steady rather than dramatic, but each step helps create the conditions for prevention to take root, for crises to reduce, and for local services to gain confidence and capacity.
Neighbourhood working will not solve every challenge, but it offers a realistic and necessary pathway toward a more balanced system. The moment calls for resolve and commitment, not because implementation is easy, but because continued delay risks increasing the long-term costs of reform.